Clinical workflow
A patient walks in with a painful red eye.
OptoGuide™ moves you from recognition to decision during the consult — separate the don’t-miss causes, decide urgency, and prepare a referral without leaving the room.
Structured for Australian optometry practice. Clinically reviewed by Dr Ankit Mathur, PhD, Grad Cert Ocu Thera, B.S. Optom.
Clinical decision support only
Red flags — assess urgently before anything else
Any of these supports same-day assessment or referral. Treat a painful red eye as a safety question until a benign surface explanation is clear.
- Moderate to severe pain, marked photophobia, or reduced visual acuity.
- Contact lens wearer with focal corneal staining, an infiltrate, or central involvement.
- Corneal opacity, an epithelial defect, a dendritic staining pattern, or hypopyon.
- Ciliary (circumlimbal) flush with cells and flare, or an irregular or fixed mid-dilated pupil.
- Severe unilateral pain with nausea, haloes, corneal oedema, or markedly raised IOP.
- Chemical exposure, penetrating trauma, or pain out of proportion to the visible signs.
One connected workflow, not separate lookups
Recognition, management, prescribing, and referral usually live in different tools. In OptoGuide™ they are one path — each step hands off to the next so the decision keeps moving.
Step 1
Start from the presentation
Begin with what the patient reports, not a label. Measure vision first, then let the pattern of redness, pain, and photophobia point to the likely site of pathology.
- Record visual acuity before instilling drops where possible — it anchors urgency.
- Read the pattern of redness: diffuse, sectoral, or ciliary (circumlimbal).
- Localise to lid margin, conjunctiva, cornea, anterior chamber, sclera, or pressure-related.
- Contact lens wear, trauma, or chemical exposure reframes the whole assessment.
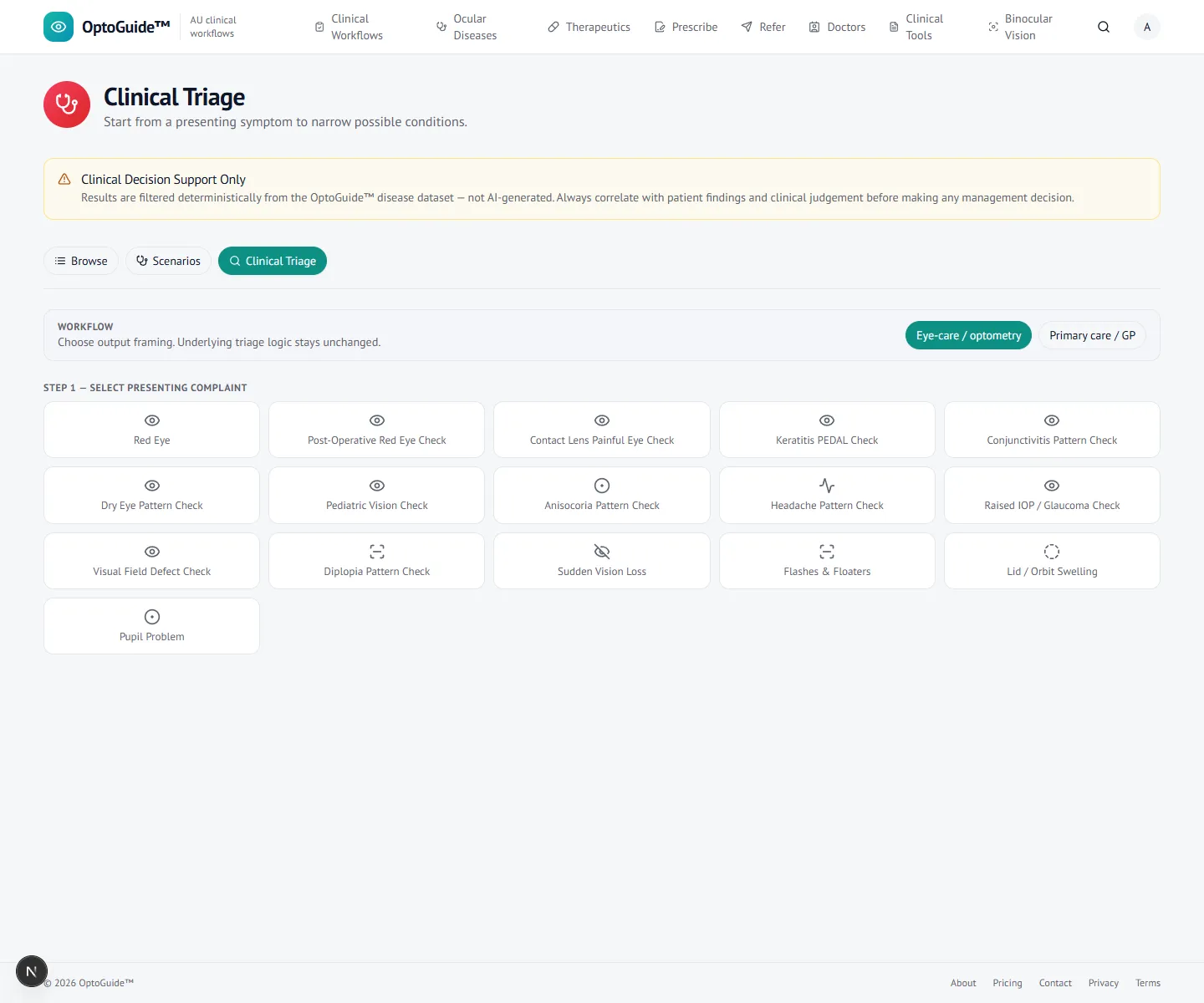
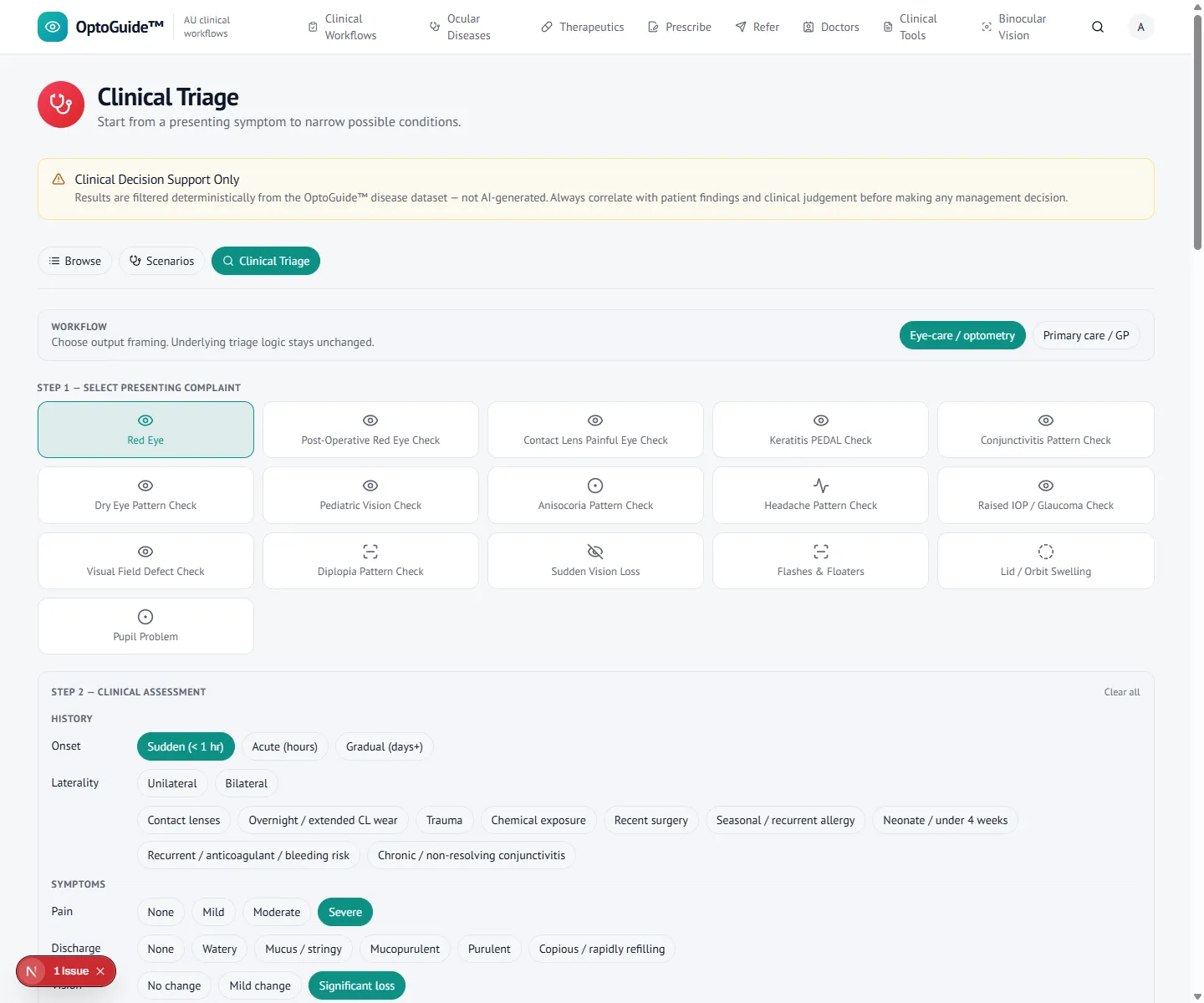
Presentation-first entry for a high-frequency, high-risk complaint. Step 2
Separate the don’t-miss causes
Keratitis, anterior uveitis, scleritis, acute angle closure, and trauma can sit behind an ordinary-looking red eye. The findings screen keeps pain, pupil, pressure, and vision in view rather than settling on conjunctivitis by default.
- A painful red contact lens eye is treated as potentially corneal until proven otherwise.
- Cells and flare with consensual photophobia raise concern for anterior uveitis.
- Deep, boring pain or pain on eye movement raises concern for scleritis over episcleritis.
- Severe pain with haloes, nausea, and a mid-dilated pupil raises concern for acute angle closure.
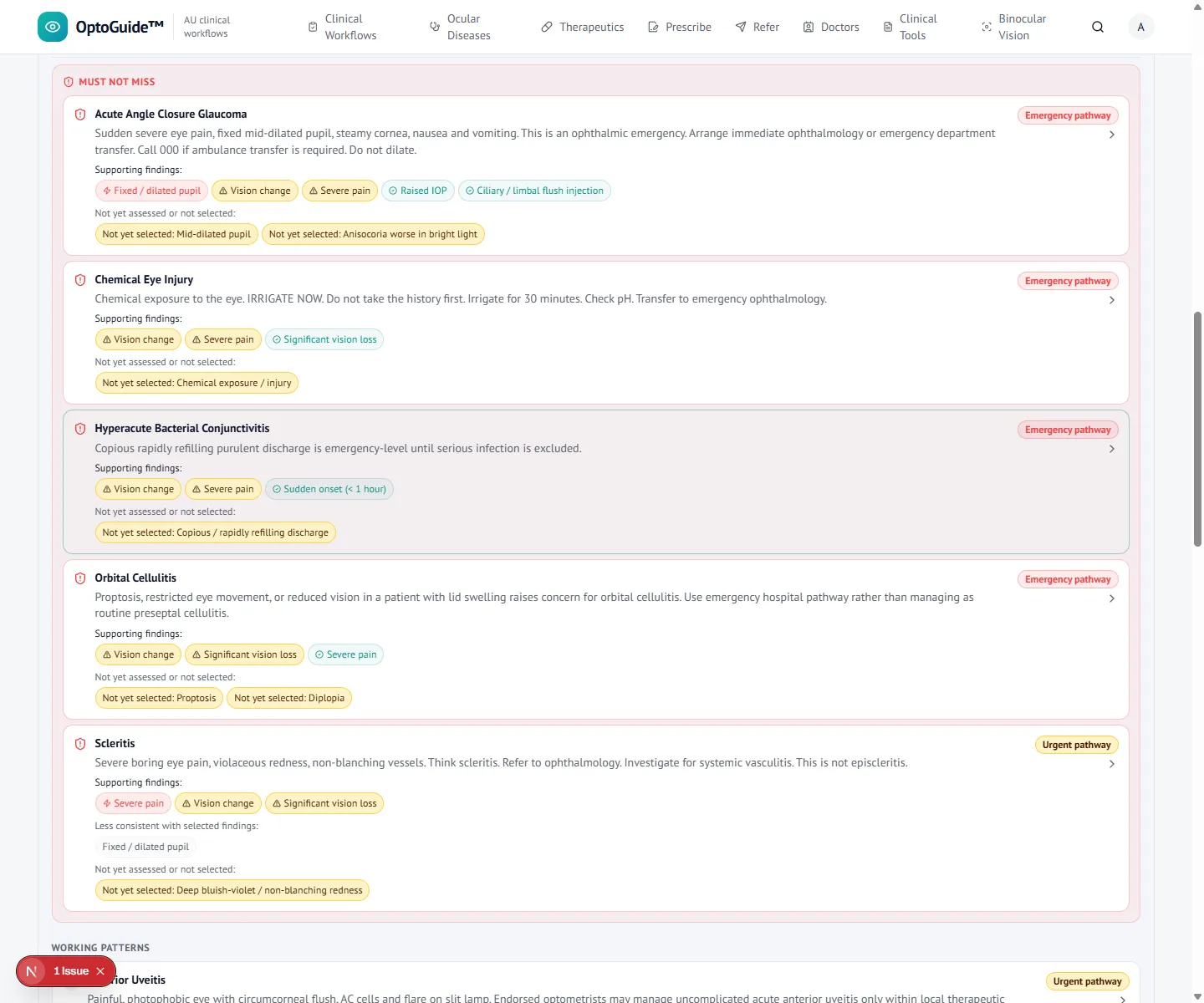
Step 3
Read the deterministic result
The findings surface a rule-based, safety-first result — not a probabilistic guess. Sight-threatening causes are held visible instead of being buried in a long list.
- Must-not-miss conditions are surfaced early, before routine explanations.
- The reasoning is transparent and rule-based, so you can sanity-check it against the eye.
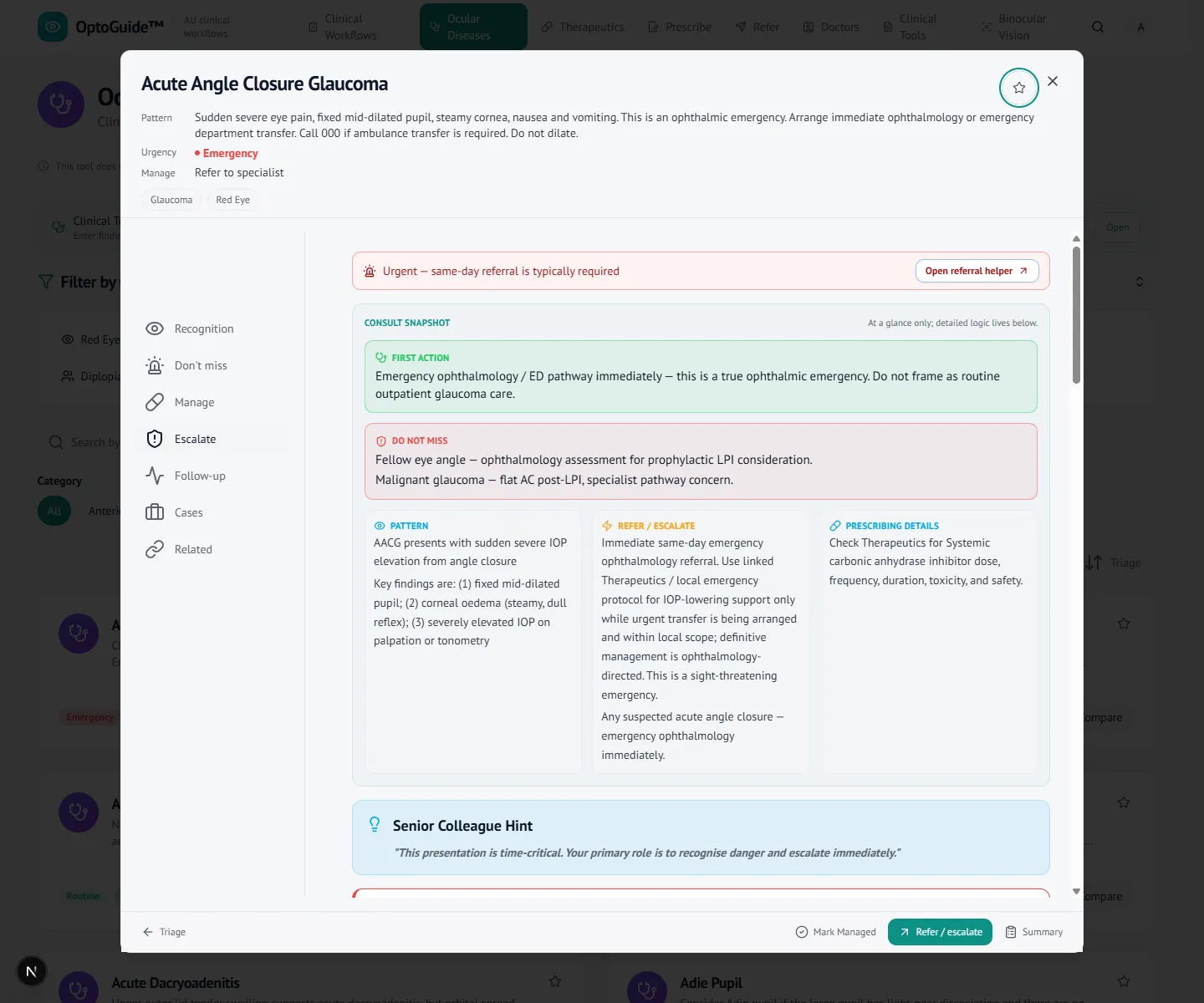
Step 4
Open the disease workflow to act
Open the fitting condition for structured recognition, risk framing, and next-step guidance. Where prescribing is clinically supported and within your endorsement, it sits alongside the decision.
- Escalate the same day when the cornea or vision is involved, rather than observing.
- Steroid decisions are weighed against herpetic risk, masked infection, and IOP response.
- Check and document IOP where safe and clinically relevant.
- Give explicit warning symptoms that should trigger immediate review.
Step 5
Draft the referral
When the eye needs ophthalmology, draft the referral in the same flow with urgency matched to the suspected diagnosis. OptoGuide generates the letter text to copy into your existing systems — it never sends on your behalf.
- Same-day wording for suspected keratitis, uveitis, acute glaucoma, or trauma.
- Recipient practice details carry through from your referral contacts.
- Copy-first output — paste into Oculo, Medical Objects, or your PMS. No patient data is stored.
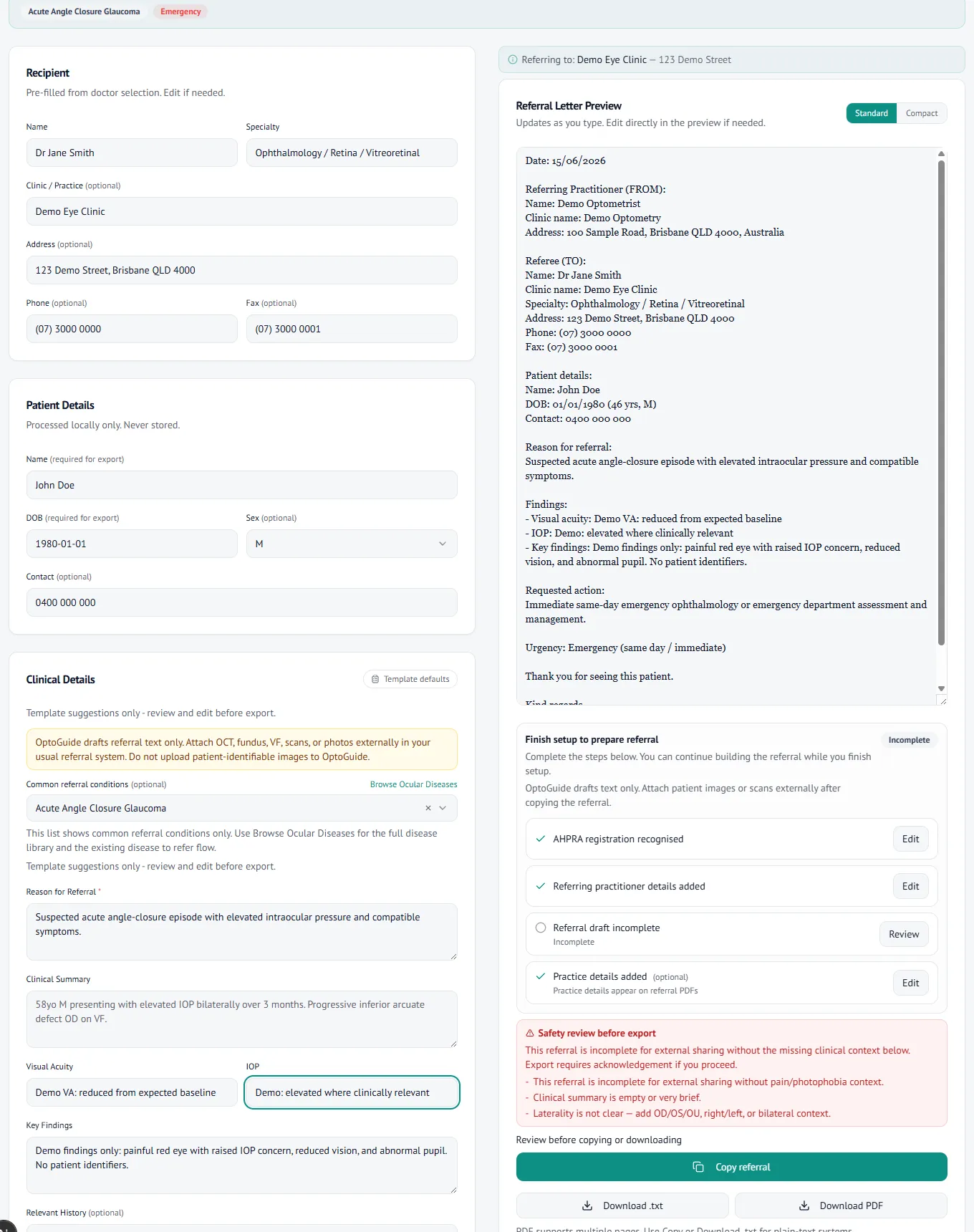
A clear emergency referral, ready for clinician review and copy.
Clinical basis
This guidance reflects standard optometric clinical reasoning based on:
- Australian optometry clinical practice patterns
- Australian medicines regulation and PBS prescribing context
- Common ophthalmology referral standards
- Evidence-based clinical training and practice
Use OptoGuide™ during the next painful red eye you see.
Free 14-day full-access trial. No credit card required.
Related clinical guides
- Red eye — differential diagnosis (optometry)
- Painful eye — differential diagnosis (optometry)
- Contact lens red eye — triage and referral
- Corneal ulcer — red flags and referral priorities
- Keratitis vs uveitis
- Episcleritis vs scleritis
- Anterior uveitis — referral priorities
- Steroid eye drop risks — key red flags and review points