Clinical workflow
A patient reports new flashes and floaters.
OptoGuide™ starts from the presentation and triages by retinal risk — the danger clues stay in front of you, and retinal tear and detachment are never buried behind a benign explanation.
Structured for Australian optometry practice. Clinically reviewed by Dr Ankit Mathur, PhD, Grad Cert Ocu Thera, B.S. Optom.
Clinical decision support only
Red flags — assess urgently before anything else
Treat symptomatic retinal break risk as time-sensitive until excluded. Same-day review is supported when the peripheral retina cannot be confidently assessed.
- A curtain, veil, or new peripheral field defect.
- A sudden increase in floaters or a dense shower of black spots.
- Shafer sign, vitreous pigment, or haemorrhage.
- A reduced view of the peripheral retina.
- Recent trauma or high myopia with new symptoms.
One connected workflow, not separate lookups
Recognition, management, prescribing, and referral usually live in different tools. In OptoGuide™ they are one path — each step hands off to the next so the decision keeps moving.
Step 1
Start with the presentation
Begin from the presenting complaint rather than a disease list. The pathway prompts the symptom features that predict retinal risk.
- Establish whether the flashes and floaters are new or changed.
- Ask specifically about a curtain, shadow, or field loss.
- Note high myopia, trauma, or recent posterior vitreous detachment.
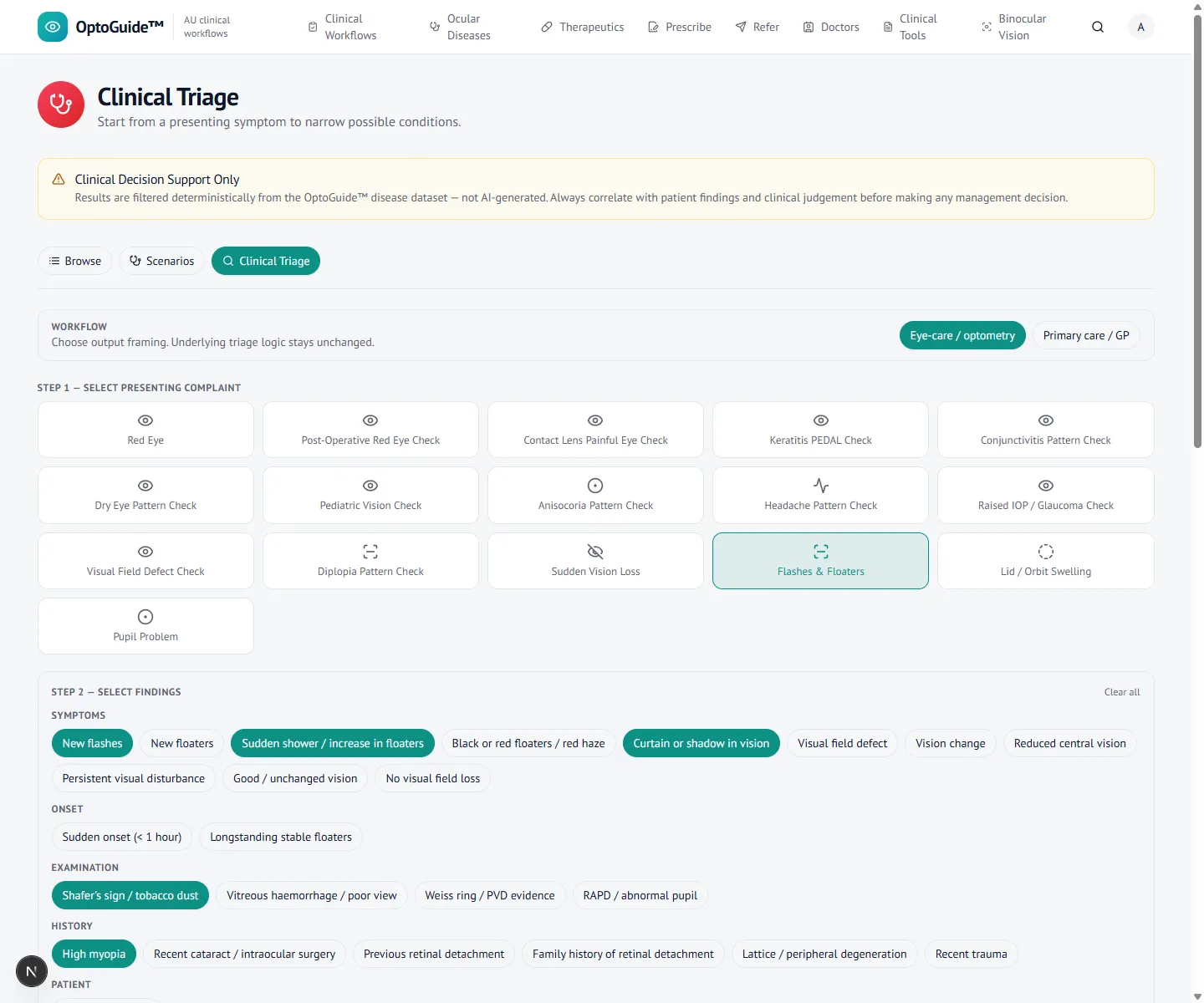
Step 2
Select the danger clues
Capture the retinal-risk findings — new flashes, a sudden shower of floaters, curtain or shadow, Shafer sign, high myopia — without any patient identifiers.
- A dense shower of floaters or Shafer sign raises concern for a tear.
- A curtain or field defect raises concern for detachment.
- A reduced peripheral view is itself a reason to escalate.
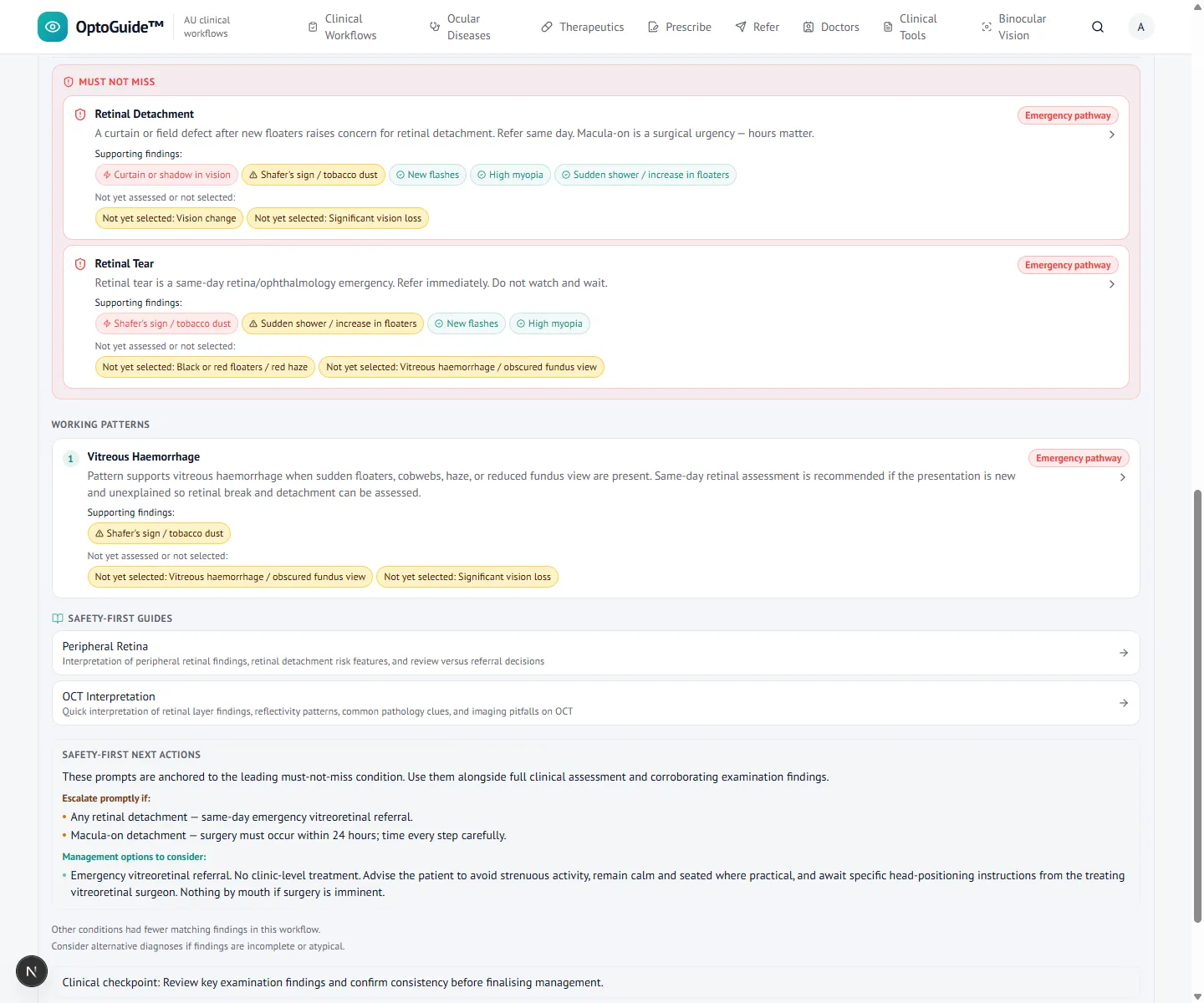
Step 3
Keep tear and detachment visible
A deterministic result separates likely benign vitreous change from must-not-miss retinal disease, holding tear and detachment in view.
- Triage is by retinal risk, not by symptom annoyance alone.
- Working and must-not-miss patterns are both shown.
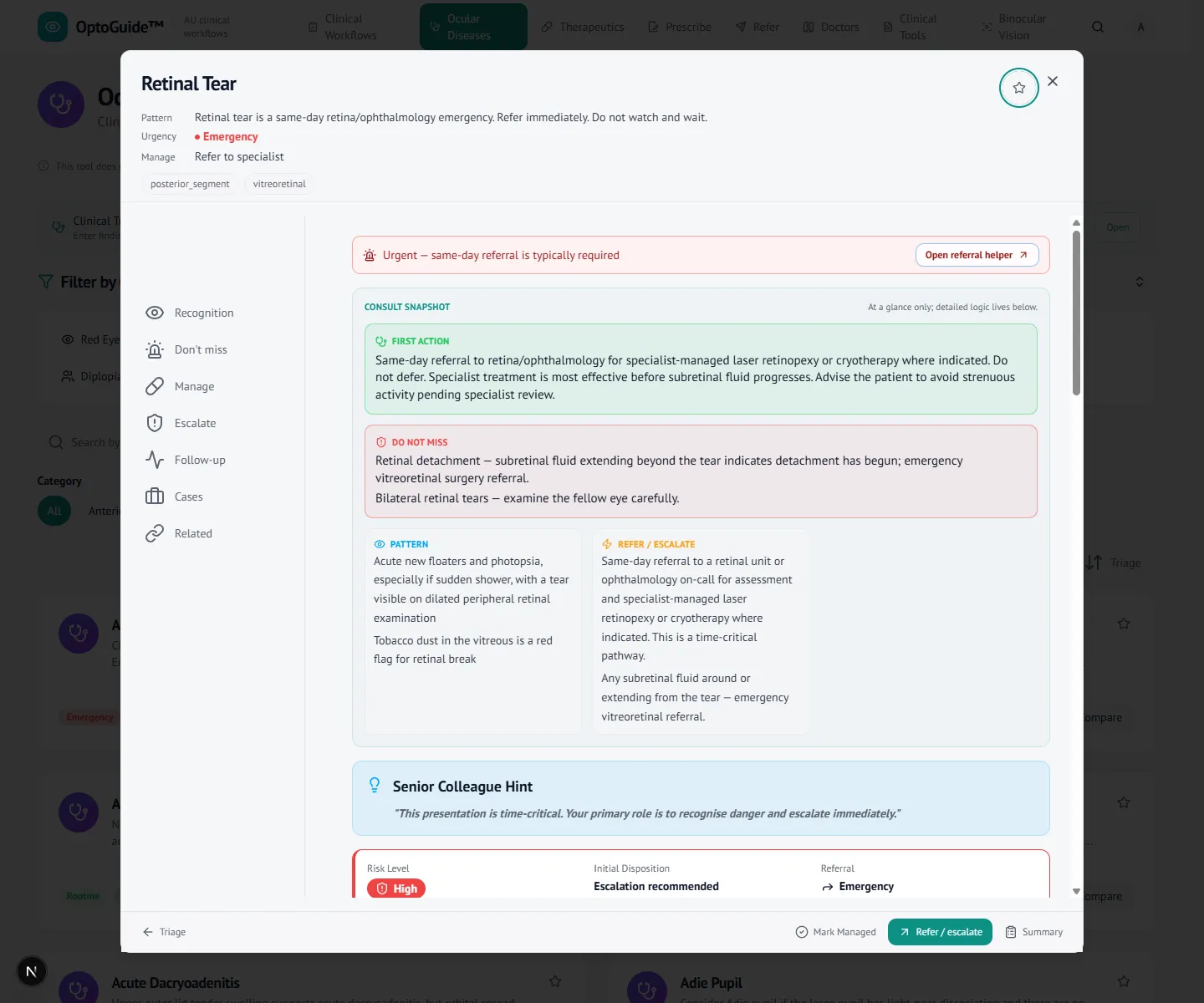
Step 4
Move to clinical action
Open the fitting condition for recognition, risk, escalation, and management. If the initial exam is benign, give strict return advice.
- Same-day escalation when a tear, detachment, or field defect is suspected.
- Explain the warning symptoms that should trigger immediate review.
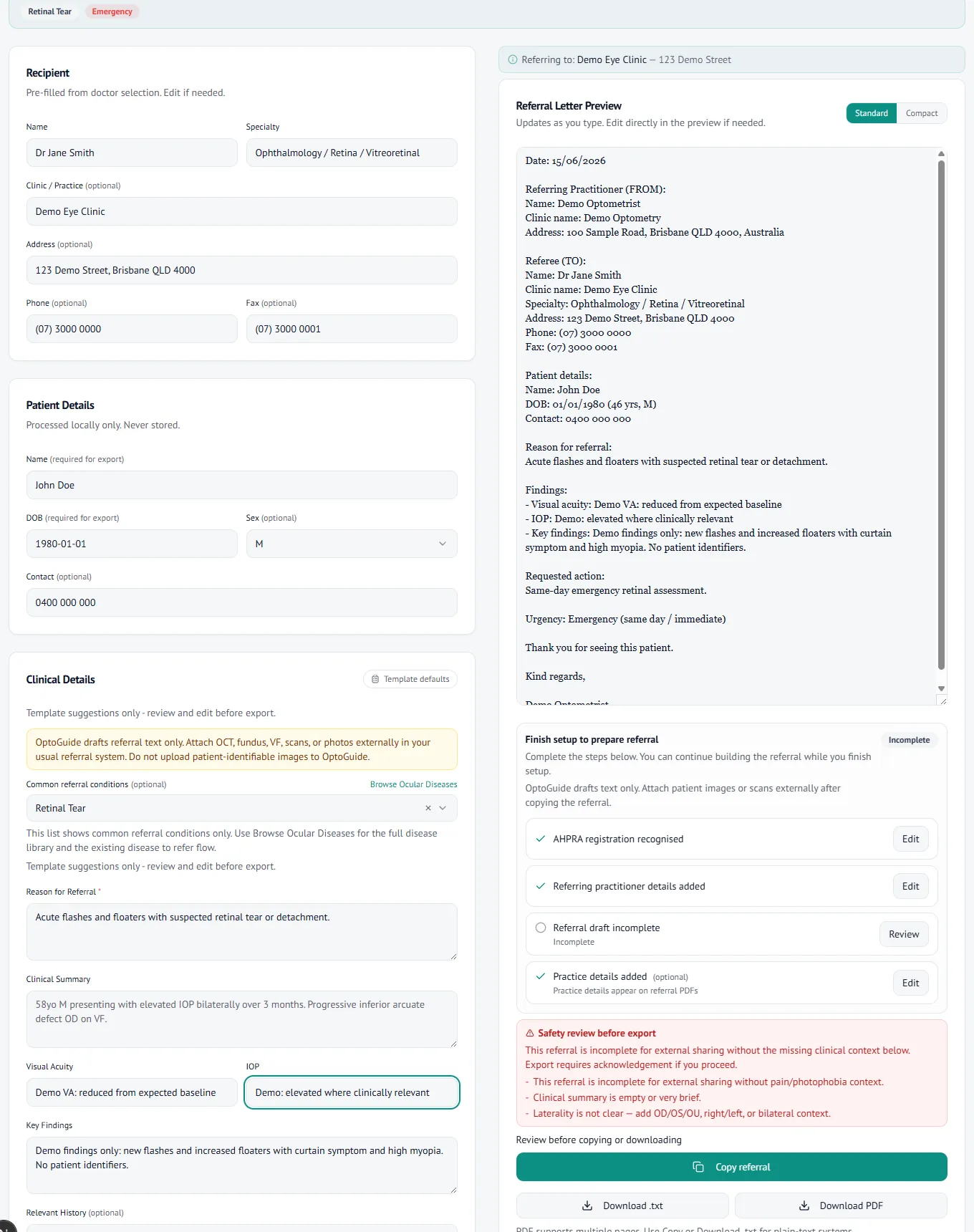
Step 5
Copy a same-day retinal referral
Draft the referral from disease context with urgency prefilled and findings clinician-entered. The letter text is reviewed and copyable for your existing systems.
- Referral urgency carries through automatically from the workflow.
- Copy-first output for Oculo, Medical Objects, or your PMS. No patient data is stored.
Clinical basis
This guidance reflects standard optometric clinical reasoning based on:
- Australian optometry clinical practice patterns
- Australian medicines regulation and PBS prescribing context
- Common ophthalmology referral standards
- Evidence-based clinical training and practice
Triage the next flashes and floaters by retinal risk.
Free 14-day full-access trial. No credit card required.