Management workflow
Dry eye is the most common thing you’ll see this week.
And most of it is yours to manage. OptoGuide™ structures triage and management so the plan is in front of you — foundations first, with clear cues for when to escalate.
Structured for Australian optometry practice. Clinically reviewed by Dr Ankit Mathur, PhD, Grad Cert Ocu Thera, B.S. Optom.
Clinical decision support only
Red flags — assess urgently before anything else
Most dry eye is optometrist-managed; these features support escalation rather than continued surface management.
- Severe constant pain or photophobia.
- Vision loss that does not clear on blinking.
- Corneal ulceration, thinning, or an infiltrate.
- Features suggesting Sjögren’s or another systemic association.
One connected workflow, not separate lookups
Recognition, management, prescribing, and referral usually live in different tools. In OptoGuide™ they are one path — each step hands off to the next so the decision keeps moving.
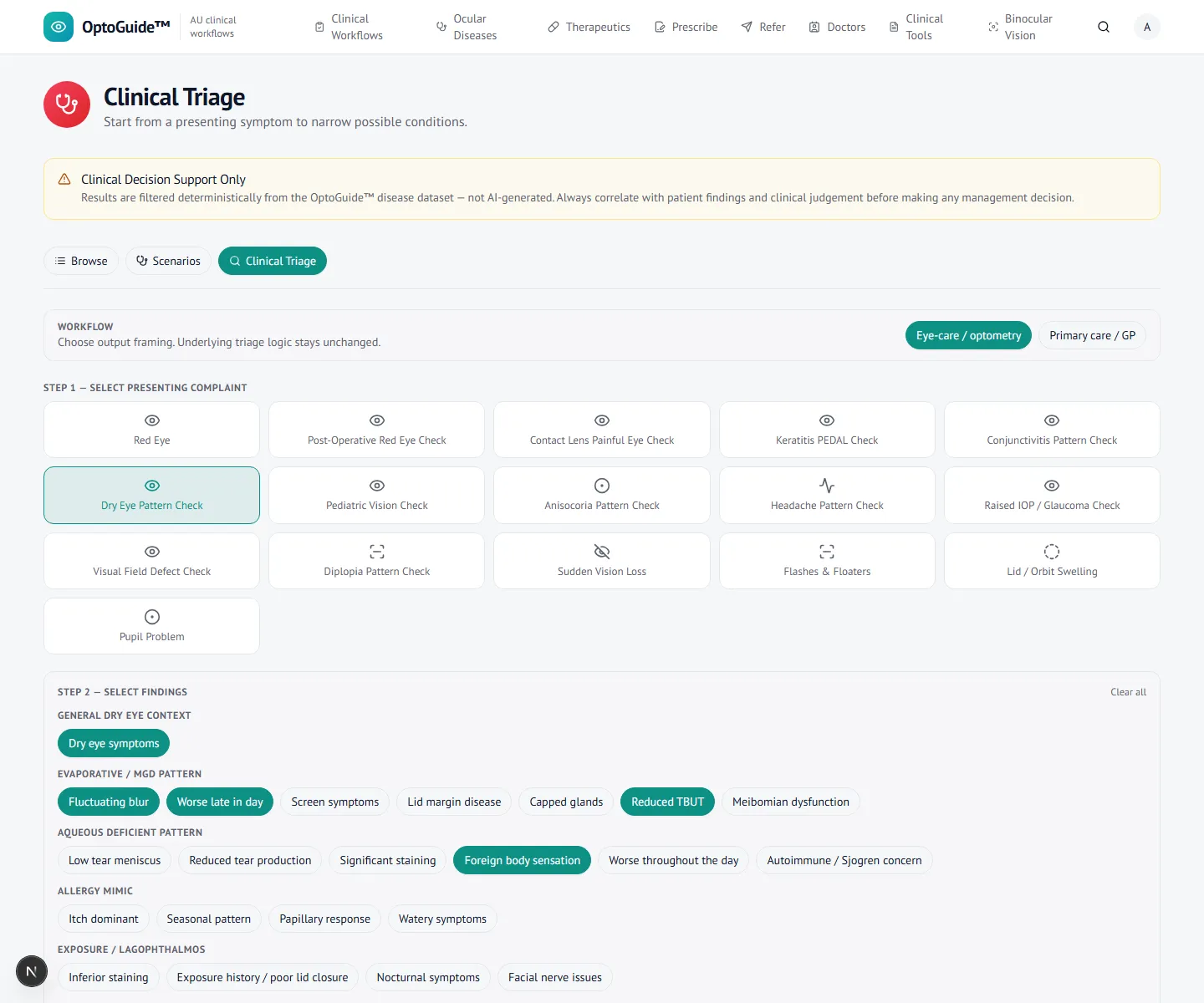
Step 1
Triage the presentation and findings
Start from the presenting complaint, then the findings — here a dry-eye pattern: symptoms worse late in the day, a reduced tear break-up time, and fluctuating blur that clears on blinking.
- Capture the features that change management, not just the symptom.
- Look for the meibomian-gland component alongside aqueous deficiency.
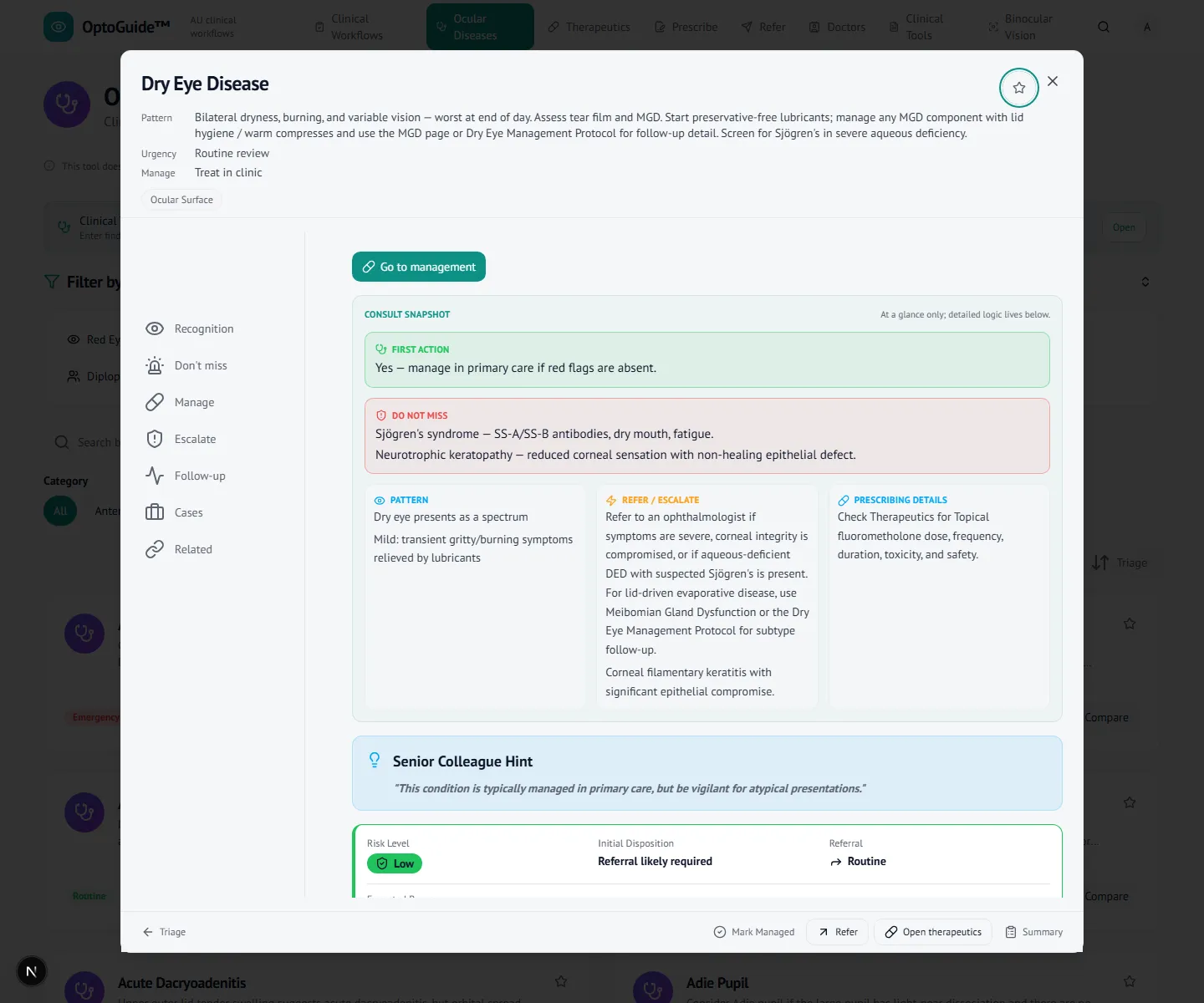
Step 2
Open the management workflow
The findings surface a deterministic dry eye / MGD pattern. Open the condition for recognition, management, escalation, and review in one view — an optometrist-led first-line plan.
- Set expectations for a chronic condition and build the foundation plan.
- Address the MGD component where present, and treat co-existing surface disease together.
Step 3
Know when to escalate
The workflow keeps the escalation cues visible so a chronic, manageable condition still has a defined path out when it changes. The clinician reviews and follows up.
- Escalate for severe pain, unremitting photophobia, or vision loss that does not clear on blinking.
- Escalate if corneal integrity is compromised, or Sjögren’s is suspected.
Clinical basis
This guidance reflects standard optometric clinical reasoning based on:
- Australian optometry clinical practice patterns
- Australian medicines regulation and PBS prescribing context
- Common ophthalmology referral standards
- Evidence-based clinical training and practice
Put the dry-eye plan in front of you at the point of care.
Free 14-day full-access trial. No credit card required.