Clinical workflow
A patient describes new double vision.
OptoGuide™ starts with the diplopia pattern, not guesswork — separate monocular from binocular double vision, capture the neuro red flags, and escalate the acute presentations that need urgent assessment.
Structured for Australian optometry practice. Clinically reviewed by Dr Ankit Mathur, PhD, Grad Cert Ocu Thera, B.S. Optom.
Clinical decision support only
Red flags — assess urgently before anything else
New acute binocular diplopia that is unexplained or neurologically suspicious supports same-day or urgent referral.
- Acute binocular diplopia with headache or neurological symptoms.
- Pupil involvement, ptosis, or painful eye movements.
- New limitation of ductions or an incomitant deviation.
- Associated facial weakness, ataxia, or sensory symptoms.
- Orbital pain, proptosis, or lid swelling.
One connected workflow, not separate lookups
Recognition, management, prescribing, and referral usually live in different tools. In OptoGuide™ they are one path — each step hands off to the next so the decision keeps moving.
Step 1
Start with the diplopia pattern
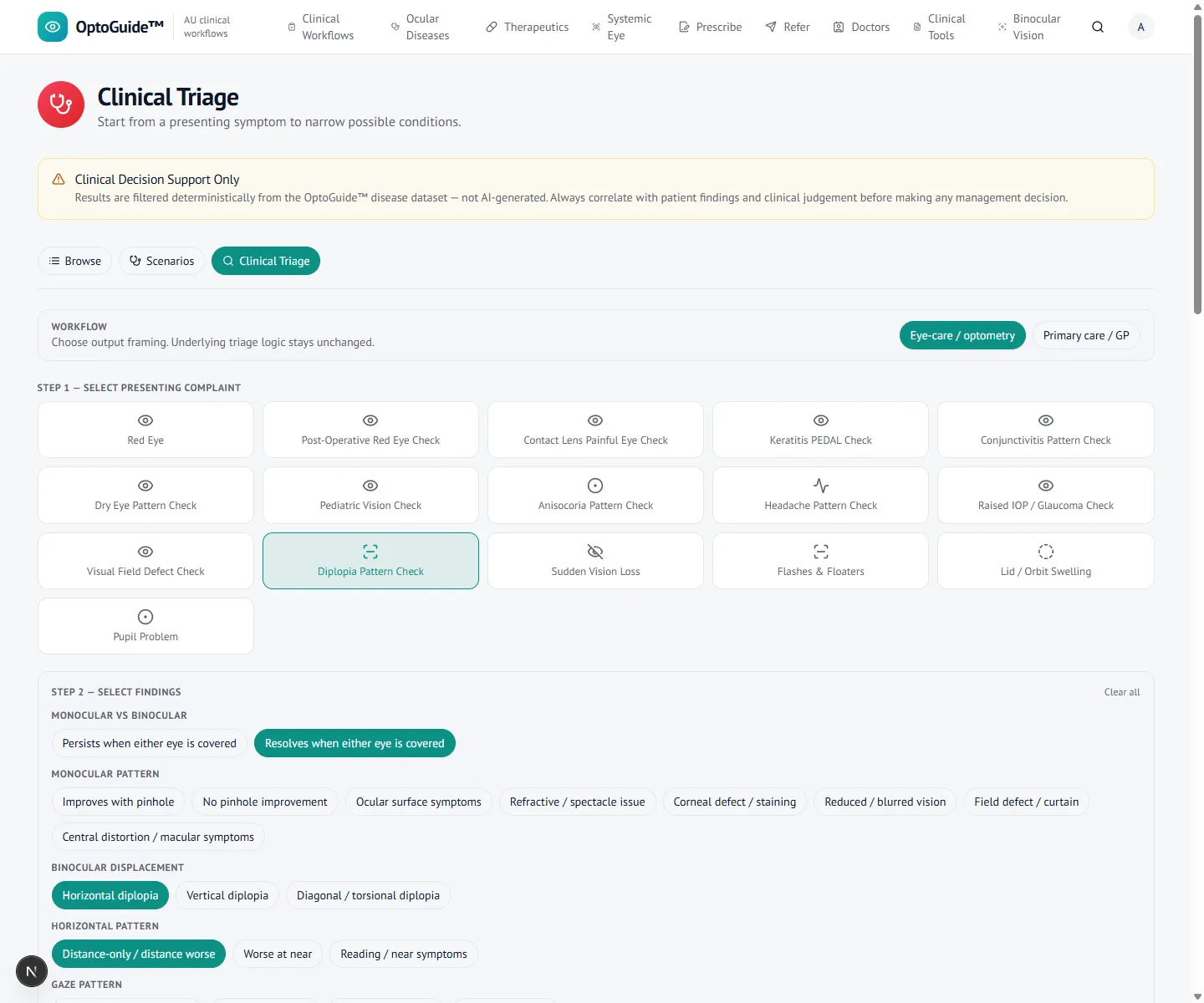
Classify the double vision before chasing a cause. The first question — does it resolve when either eye is covered — separates monocular from binocular diplopia.
- Monocular diplopia persists with one eye covered and is usually optical.
- Binocular diplopia resolves when either eye is covered and is the neuro-ophthalmic concern.
- Note direction (horizontal / vertical), onset, and distance vs near.
Step 2
Capture the neuro red flags
Capture the motility and neurological cues that change urgency — an abduction deficit, incomitance, vascular risk factors, headache, or associated neurology.
- A horizontal deficit worse at distance can reflect a sixth nerve palsy.
- Pupil involvement or ptosis with diplopia is a red-flag combination.
- Acute onset with vascular risk factors is captured explicitly.
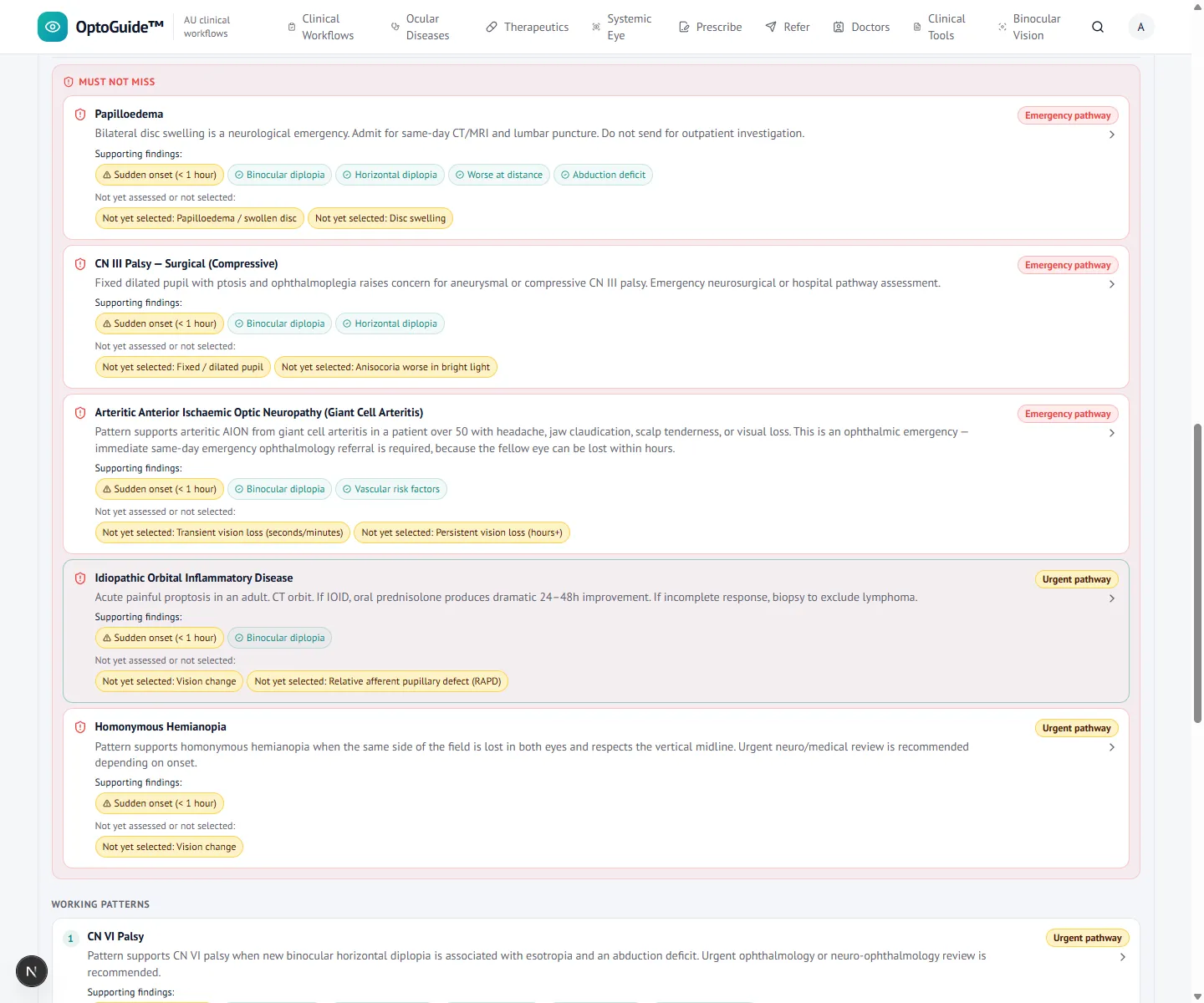
Step 3
Keep acute neuro causes separate
A deterministic result keeps acute neuro diplopia out of the routine binocular-vision pile, surfacing cranial nerve palsies and must-not-miss causes.
- Routine BV imbalance and acute neuro diplopia are not mixed together.
- Must-not-miss neuro causes are held visible for escalation.
Step 4
Open the action workflow
Open the fitting condition for structured recognition and referral cues. New acute binocular diplopia is escalated rather than observed without explanation.
- Recognition and escalation framing are conservative — no cause is asserted.
- Document motility findings and any neurological association clearly.
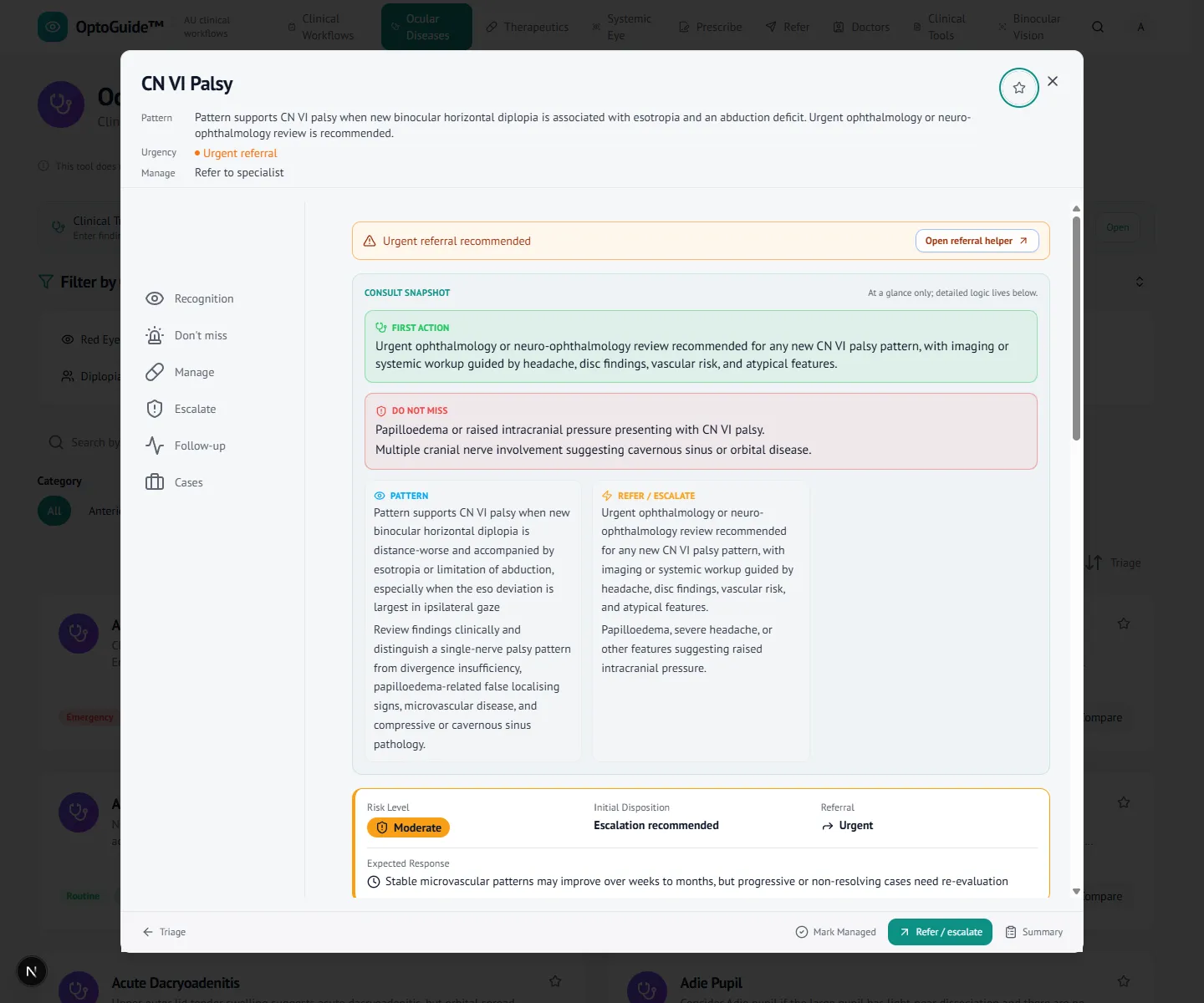
Step 5
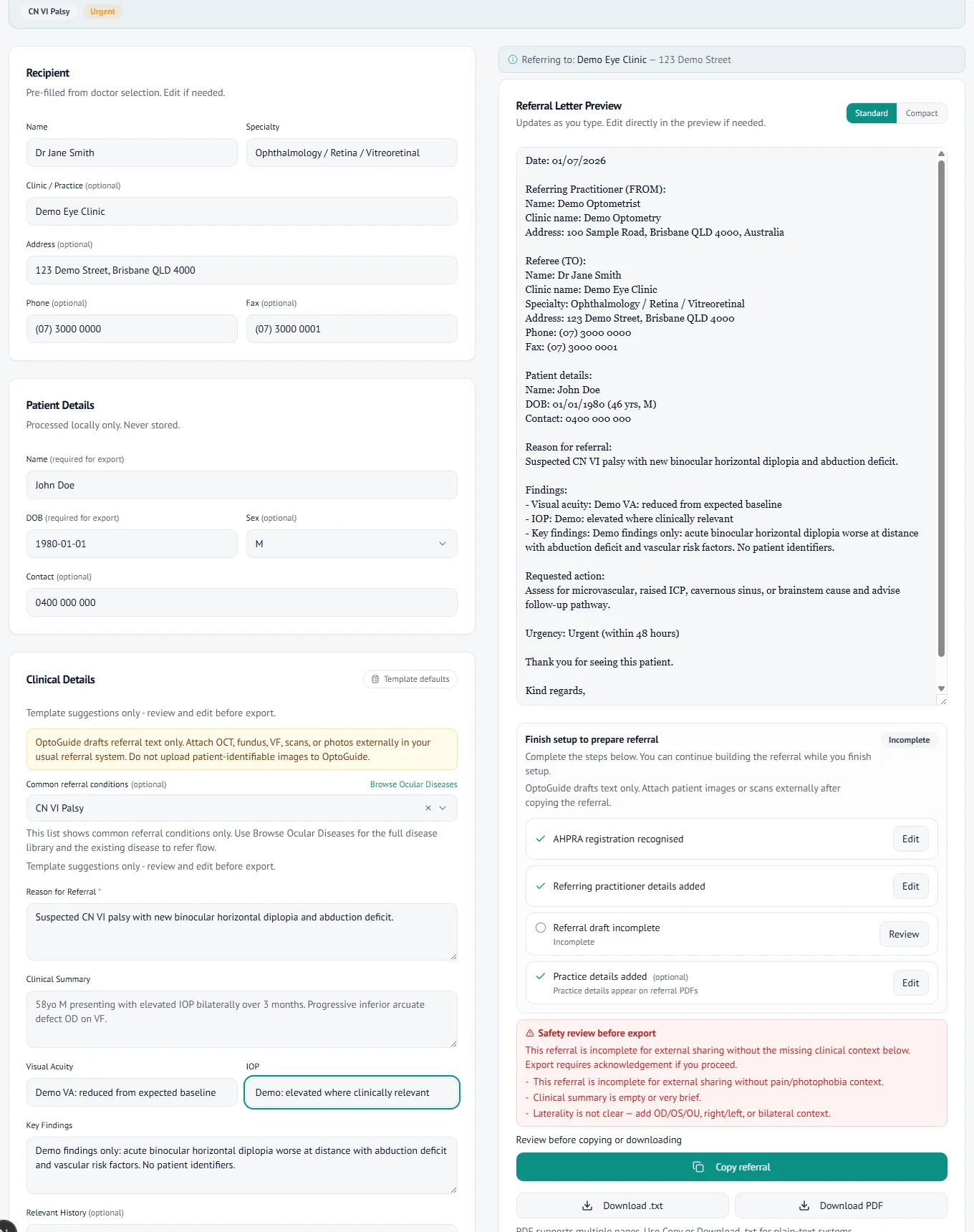
Draft an urgent referral
Draft an urgent neuro-ophthalmic referral from the workflow, with urgency prefilled and findings clinician-entered. The letter is generated for you to review and copy.
- Urgent neuro-ophthalmology wording from the clinical pathway.
- Copy-first output for your existing systems. No patient data is stored.
Clinical basis
This guidance reflects standard optometric clinical reasoning based on:
- Australian optometry clinical practice patterns
- Australian medicines regulation and PBS prescribing context
- Common ophthalmology referral standards
- Evidence-based clinical training and practice
Start the next case of double vision with the pattern.
Free 14-day full-access trial. No credit card required.